IEEE TRANSACTIONS ON NUCLEAR SCIENCE
Antonio J. Gonzalez, Member, IEEE, David Sanchez, Santiago Jimenez-Serrano, Alvaro Anreus, Edwing Ulin-Briseño, Andrea Gonzalez-Montoro, Member, IEEE, Marta Freire, Luis F. Vidal, Marc Gil, Jorge Alamo, Julio Barbera, Alvaro Mondejar, Alfonso Rios, Jose M. Benlloch, Adela Sara Canoves Llombart, Begoña Martinez Sanchis, Irene Torres-Espallardo
Abstract
Total Body – PET is becoming more popular these days, with about 50 systems already installed worldwide, with axial coverages ranging from 100 to 200 cm, including timing capabilities in the range of 180 – 250 ps. These systems have shown great potential in several application fields, due to their significantly increased sensitivity (both physical and efficient), and to the possibility to study correlations between distant organs. However, they are very expensive, and they are not enabling depth of interaction (DOI) information.
In this work we present a unique TB-PET with sufficient 70 cm axial coverage to image most relevant organs in a high percentage of the world population, combined with the DOI capabilities, improving spatial resolution performance when moved away from the scanner center. We have compared our current results with state-of-the-art TB-PET scanners, showing a factor 2-3 better performance at 30 cm off-radial positions. First clinical images have been already acquired. They are also pinpointing the advantages of improved impact determination (both monolithic and DOI directions), better delineating small and multi-centric tumors.
Index Terms — TB-PET, DOI, TOF, Clinical results.
I. INTRODUCTION
Total Body – Positron Emission Tomography (TB-PET) systems are very attractive given their unique feature of a long axial field view (FOV). This allows for a significantly increased in system sensitivity and, thus, to reduce the patient dose, scanning time, or a compromise between both. There exist two systems that are commercially available. The Vision Quadra from Siemens [1] and the new Panorama system from United Imaging [2]are feature about 1 meter and 1.5 meters axial FOV. The PennPET is also reaching about 1.5 meters but is a research system [3]. All of them are based on pixelated crystal arrays without depth of interaction (DOI) information, but with a time of flight (TOF) in the range of 180-250 ps.
In this work we present part of the performance, and the first clinical results of a unique TB-PET, named IMAS, simultaneously enabling TOF and DOI capabilities, with an axial FOV of 70 cm. IMAS is installed at the largest hospital in our region: La Fe hospital.
II. Materials and Methods
A. System description
IMAS is based on the novel semi-monolithic scintillator geometry. The scanner has a diameter of 82 cm and, and 70 cm axial coverage by assembling 5 rings of 10 cm length each, with 5 cm gaps. The main detector units are composed of LYSO mini-blocks of 8 slabs of 25×3×20 mm3 coupled to an array of 8×8 SiPMs. The slabs geometry allows one to simultaneously retrieve the DOI and TOF information. The identification of the impacts of the annihilation photons is done using Neural Networks (NN) [4][5]. The IMAS detector includes novel multiplexed readout electronics that reduce the number of signals as more as a factor of 4, without almost impacting the performance. We have arranged 4×4 mini-modules in super-modules (SM), and each ring is composed of 24 SM (see Fig. 1). IMAS is installed together with a standard CT. IMAS has been characterized mainly following the NEMA 2018 protocol.
We are reconstructing images using both MLEM or OSEM algorithms accelerated by GPU, being the second about 3 times faster without compromising image quality. Most of the images are reconstructed using 10 OSEM iterations and 5 subsets, resulting in a 3D image comprising 391× 391×346 cubic voxels of 2.06 mm.
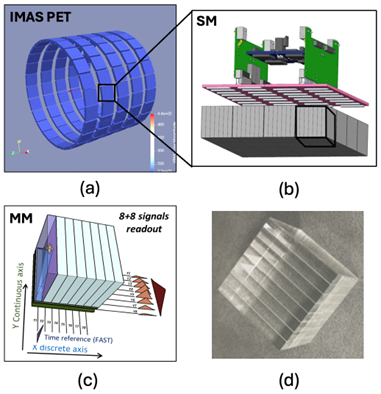
Fig. 1. (a) Sketch of the IMAS PET equipment consisting of 5 rings (b) Sketch of a SM with the readout system; (c) Sketch of a MM with its 8 time and 8 energy channels; (d) Photograph of the MM with 1´8 LYSO slabs.
B. Clinical tests
A clinical validation is currently undergoing with patients that are programmed for a conventional PET/CT. In particular, we compare our results with those obtained with the PET/CT Philips Gemini TF. Few patients have been already scanned, first in the PET/CT and later in IMAS. Although IMAS counts with a CT, we have currently used the CT of the Philips PET/CT for attenuation correction on the IMAS using deformable models. The reason for this is simply to avoid any additional radiation before we are fully confident on the IMAS performance. To co-register our PET with the Philips CT, we employed a method based on calculating deformation matrices through geometric transformations, formulated as an optimization problem that iteratively adjusts transformation parameters to align both images. The patient was measured at the conventional PET/CT with an activity of 5.8 mCi, and about 90 min later at the IMAS.
Fig. 2 a). Photograph of the IMAS PET system aligned with a GE CT

Fig. 2 b). Photograph of one imaged patient
III. Results and Discussion
Pilot results of the IMAS performance have shown an unprecedented homogeneous spatial resolution across the entire FOV with 3.7 mm at 1 cm offset, and just degrading by 1 mm at 30 cm radial position, see Fig. 2. This is obtained because of the use of accurate DOI information during the reconstruction process. When comparing these results with published works of current TB-PET systems [1][3][2], the performance of the IMAS is about 1.5-2 fold better at 20 cm off-radial, and we estimated 2.5-3 fold at 30 cm. That is, other systems could degrade to 7-9 mm FWHM.
The sensitivity of the scanner resulted in 44 cps/kBq following the NEMA protocol, and placing a source at the center of the scanner we measured a peak sensitivity of 7.6%. That is about 4-5 times larger than existing conventional PET-CT scanners. The system TOF has been determined to be 480 ps, but an improvement close to 350 ps is reachable after a more accurate time skew calibration.
Regarding image quality, we made use of the torso phantom with an activity ratio of hot-to-background of 8. Images were reconstructed with preliminary versions of normalization, random correction and TOF information. We observed that the axial views suffer from some artifacts, related to the gaps in between rings. However, the transaxial views show very good performance. Percentage contrasts above 70% were observed for the largest spheres. We expect to boost this value to nearly 80-90% by improving the normalization procedure, as well as scatter and random corrections, and finally by including a more accurate TOF during the reconstruction. Clinically, the preliminary image quality seems to be superior to the conventional PET/CT. In one of the patients, in which a multi-centric lesion was observed in the axilla, it was clearly resolved with IMAS, but blurred with the PET/CT. Figure 4 shows the comparative results of this patient, with a zoom in to this lesion area.
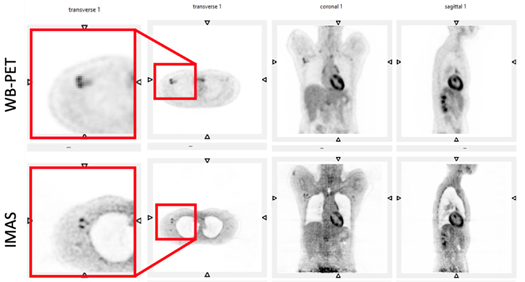
Fig. 4. Comparative image of a patient (female, 47 years and 51 kg weight), when scanned in the WB-PET Philips Gemini TF (top) and at the IMAS (bottom).
IV. Conclusions
In this work we summarize some of the performance parameters of the unique TB-PET system that simultaneously enables TOF and DOI. IMAS is a system that saves part of the cost, when compared to other existing TB-PET, by using an architecture including gaps. The unique feature in clinical PET scanners enabling DOI, results in a homogeneous spatial resolution better than 4 mm in the whole FOV. At 30 cm off-radial position, this is about 2-3 times better than any other system. We have started scanning patients at the La Fe hospital in Valencia. The increased sensitivity and accurate impact determination, significantly improve the diagnostic prediction when compared to conventional PET. Notice that we have currently used the CT of the PET/CT acquisition for attenuation correction purposes on the IMAS PET, as a first stage only to avoid extra radiation. A study we want to also report on this work is about the reduction of the IMAS CT dose, without impacting the IMAS PET performance.
References
[1] G.A. Prenosil, et al., J. Nucl. Med. 63:476–484, 2022.
[2] H. Zhang, et al., J. Nucl. Med. 65:1974–1982, 2024.
[3] B. Dai, et al., Phys. Med. Biol. 68, 095007, 2023.
[4] M. Freire, et al., Phys. Med. Biol 67, 245011, 2022.
[5] J. Barrio, et al., IEEE Trans. Rad. Plasma Med. Scie. 7, 785, 2023.
A.J. Gonzalez, S. Jimenez-Serrano, A. Anreus, A. Gonzalez-Montoro, M. Freire, E. Ulin-Briseño, L.F. Vidal, M. Gil and J.M. Benlloch, are with the Instituto de Instrumentación para Imagen Molecular (I3M), Centro Mixto CSIC—Universitat Politècnica de València, 46022 Valencia, Spain (e-mail:agonzalez@i3m.upv.es).
D. Sanchez, J. Alamo, J. Barbera and A. Mondejar are with Oncovision SA, 46022 Valencia, Spain.
A. Rios is with Full Body Insight, Valencia, Spain.
I. Torres-Espallardo, A.S. Canoves Llombart and B. Martinez Sanchis are with Hospital La Fe 46026 Valencia, Spain.

